Are the autism epidemic, toxins in vaccines, biological control systems, and human language related? Yes, they are. In this post I will show how and why they are necessarily related. It turns out that everything depends on true representations.

Albert Einstein understood this to be the case in the sciences. Did he already know in 1941 the consequences of the powers to be unleashed by his famous equation,  ? He wrote, “Everything depends on the degree to which words and word-combinations correspond to the world of impression” (1941, in Oller, 1989b, p. 62).
? He wrote, “Everything depends on the degree to which words and word-combinations correspond to the world of impression” (1941, in Oller, 1989b, p. 62).
True representations form the basis for scientific knowledge and for the development of sound theories. That much is obvious. True reports about experience also always involve events that unfold over time giving ordinary truth a narrative aspect.
It is not at all obvious, however, that ordinary true narrative representations (TNRs) in biological systems provide the essential basis for functional biochemistry, a strong immune system, a healthy gut, body, brain, and so forth. Coherent TNRs are also necessary to functional social systems, medicine, law, education, government, and economics.
Ordinary Truth
What, for example, is an ordinary true representation? Suppose I told my wife last night that this morning I would change some flourescent lightbulbs and blow out the garage and the outside porches and that in fact this morning I did so. My promise would turn out to be the basis for this true report, and it is true. I did as promised.
The truth, however, does not reside in the facts—that is, the bulbs, the light fixtures, the ladder, the clothes worn and tossed in the wash, the number of times I had to go up and down the ladder, the leaves in the garage and on the porches. The material world cannot be false. It is what it is. As important as the facts are, they merely are what they are. My reporting what they are does not change them by an infinitesimal particle. I cannot go backward in time and alter those truly reported facts in any way. Ordinary truth is not in the material facts or events as such. They just are what they are. My promise did not alter those facts either in spite of the fact that it helped to shape my own behavior toward them. The facts could have been the same without the promise and my reporting of those facts would still be true now.
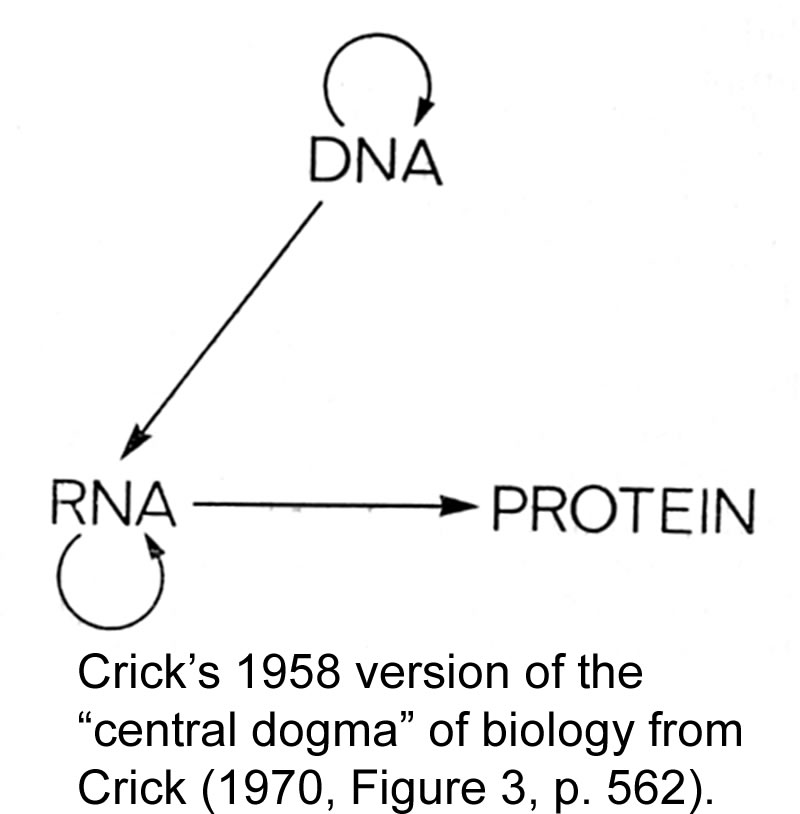
Truth is in the reporting of facts. It is in TNRs. It consists of the agreement between the representation, the TNR, and the facts. Every TNR has three parts: (1) it has symbols (such as the sentences of a language or the genetic sequences of DNA); (2) it has indexical actions (like the speaking of a speaker or signing of a signer or the reading of DNA to form RNAs); and (3) it refers to some objective facts (such as a sequence of events, or a sequence of amino acids in a protein). If these three components agree with each other, the representation is a TNR. It has ordinary truth. Keeping in mind that a person “telling the truth” may be in error, it follows that truth resides only in the representation itself. The facts referred to may change. The porches will get dirty again and the bulbs will burn out. BUt a TNR, if it is one, is eternally indifferent to such changes. Its truth value is unaffected by subsequent changes in the facts. Therefore, the truth does not reside in the facts.
For example, on account of the way I put my report together by my use of language about the porches, bulbs, and so forth, the report is true of those facts. But the truth is not in the facts, it is strictly in the report.
Any facts (and there always exists an infinite variety of them at all times) just are whatever they are. They cannot be false. They cannot be fictional. They cannot err. They cannot lie. And, they can never remain completely unchanged.
Representations are different. They can be true, fictional but meaningful, wrong innocently as in errors or deliberately as in lies, and they can also be nonsensicial as in mere babbling. Suppose right now I say I am sitting at my computer and I am. That statement would be a TNR. If I said I am driving my car, that would not be true because at this moment I am working in my study at home.
Similar representational phenomena can be found in biological systems which also depend on “truth” in the ordinary mundane sense. To show why and how this is so requires some abstract theory but it is not very difficult to think through.
Biological TNRs
In biology, if a sequence of codons in DNA calls for a certain sequence of amino acids in a protein and through a long and complex cascade of dynamic interpretive systems that particular sequence of amino acids is constructed by the ribosome, the outcome would be the formal equivalent of a TNR. Commonly we think of true reports as coming after the fact, but except for the timing of the report itself, the “truth” relation is identical in a promise fulfilled and a true report given after the fact.
The strictest mathematical logic shows, and empirical science confirms, that disrupting TNRs in biological systems ultimately results in disorders, diseases, injuries, and mortality. This holds for all representational systems without exception from genetics to human languages. It holds for every kind of organization that TNRs make possible in biological and social systems. Without TNRs there would be no biosphere, no human languages, and none of the systems of law, government, commerce, education, and so forth that we depend on as human beings. All representational phenomena depend for their very existence on TNRs. This has been strictly proved in more than one way.
For a technical paper providing the theoretical basis and summing up the crucial relevance of TNRs for biological systems, see Entropy 2010. To understand the power of the full arguments given there, it is necessary also to consult the references in that paper. For anyone interested in some of the peculiar mathematical difficulties facing the 19th century orthodoxy, also see the papers linked at Evolutionary Informatics.
For a nontechnical explanation showing why everything depends on TNRs, absolutely everything, keep reading this post and the narrative that follows. It sums up the key findings of a series of theoretical works and scientific papers showing how undesirable biological and social consequences flow inevitably from incomplete, damaged, and sometimes deliberately falsified representations. However, no false representations of particular facts (errors) can be discovered except by comparing them against TNRs.
 For instance, was Archaeopteryx (at the right) a transitional form between reptiles and birds? Or was this specimen a fully feathered bird? Fred Hoyle complained that “there are no steps in the record from reptiles to Archaeopteryx or from Archaeopteryx to birds, as the Darwinian theory requires” (1983, p. 43). Was the lithograph shown here tampered with? A fradulent made-up fossil? It’s a moot question if Hoyle’s argument stands, and it does. Whether it is a flying bird or not, it certainly is very different from reptiles and if the feathers were faked, as some have claimed in recent years, then it was not much of a bird either. No matter, there are no transitions leading to it or from it in either direction. Case closed.
For instance, was Archaeopteryx (at the right) a transitional form between reptiles and birds? Or was this specimen a fully feathered bird? Fred Hoyle complained that “there are no steps in the record from reptiles to Archaeopteryx or from Archaeopteryx to birds, as the Darwinian theory requires” (1983, p. 43). Was the lithograph shown here tampered with? A fradulent made-up fossil? It’s a moot question if Hoyle’s argument stands, and it does. Whether it is a flying bird or not, it certainly is very different from reptiles and if the feathers were faked, as some have claimed in recent years, then it was not much of a bird either. No matter, there are no transitions leading to it or from it in either direction. Case closed.
But is any of this discussed in the biology books recently recommended by BESE for adoption by Louisiana high schools? Archaeopteryx, long the index fossil of the whole story, is only discussed in ways that would leave the 19th century dogma in tact. No wonder Gould admitted that the claims for transitional fossils were based on wishful thinking. Colin Patterson, senior paleontologist at the British Museum of Natural History in London commented in a 1981 interview:
… all one can learn about the history of life is from systematics , from the groupings one finds in nature [make that 19th century philosophy applied liberally to living species and to fossils in what Gould called the “Cambrian explosion”]. The rest of it is story-telling of one sort or another. We have access to the tips of the tree; the tree itself is theory, and people who pretend to know about the tree and to describe what went on it—how the branches came off and the twigs came off—are, I think, telling stories (p. 390).
Connecting the Dots
Are the autism epidemic, the controversies surrounding the toxins in vaccines, biological control systems, and the unique human language capacity related to the contents of the Louisiana biology books? Are they related to the social systems of medicine, law, government, and education? Indeed, they are, but the connections are not entirely obvious until we spell them out.
In serving as a research professor at the University of California in Los Angeles, at the University of New Mexico in Albuquerque, and more recently at the University of Louisiana, for 42 years, in my published scientific theoretical and empirical work, I have confirmed that narratives told in a chronological order are the simplest kind, the easiest to construct, and to interpret. So, that is the way I will present the argument to be developed in this post. The argument as presented is both an instantiation of a TNR and an explanation of why ordinary truth as exemplified is so important in biology, the sciences at large, and in social systems.
Start the Clock in 1968
Based on my first encounter with “linguistics” (the scientific study of language, falling more or less between mathematics and psychology), I had noticed a gap in understanding that I knew how to fill. The main missing element in the theories that were widely accepted in the 1960s (from about 1933 forward), especially in America, was attention to the real world of experience.
Leonard Bloomfield (1933) had argued that the study of meaning would be too difficult to analyze and understand, he supposed, because of the infinite variability of the contexts of experience. He proposed to concentrate his attention on the surface forms of language, its sounds (phonemes) and sequences of them. He not only had narrowed attention down to just the symbols of language, but he threw away any hope of producing a sensible theory of how children develop their first language and become readers. In the middle 1950s, Chomsky’s teacher, Zellig Harris perpetuated Bloomfield’s error by insisting that it ought to be possible to discover everything worth knowing about the “structure” of any language, by merely examining the “distribution” of its surface forms relative to each other.
Chomsky (1957) stepped back a little from that “discovery procedure” but continued to balk at the idea of bringing meaning and the real world into play. He would continue to hold for many years to come that the real world has no special place in the acquisition of language or in his theory of grammar (Chomsky, 1995). From my first experimental studies forward (Oller & Obrecht, 1968, 1969; Oller & Sales, 1969) and in my first theoretical papers (Oller, Harrington, & Sales, 1969; Oller, 1970), I argued that connections of linguistic forms with particular facts in the contexts of experience unfolding over time are essential to language acquisition and comprehension.
I got the idea from my father’s Spanish language program, El español por el mundo (Oller, Sr., 1963-1967) which illustrated the importance of the “meaningful sequence” of ordinary experience, its narrative aspect, in providing the necessary and sufficient framework for language acquisition. That program remains, according to historian of educational films,Geoff Alexander, “one of the most extensively researched and produced foreign language instruction films ever made” and is distinguished in being “based on a continuous narrative.” (Here is one of the films, the 54th in Level 1 of the 3 level program with 101 films in the whole sequence, so that readers can get an idea of the depth and complexity of language attainable even in a foreign language classroom.)
A first step toward correcting Bloomfield’s error was the development of the idea of “pragmatic mapping” (well illustrated in the Spanish program just referred to)—the process by which TNRs are constructed. The idea was under construction for a while beforehand but was published, I believe for the first time, in Oller (1975). It is an idea that is now in the mainstream being used refer to referential processes in general. The key problem in pragmatic mapping is how to associate any given referring phrase, say, for instance, Álvaro, in the film linked to the previous paragraph, with the person named “Álvaro” and referred to in that way and through other phrases (such as, “el hermano mayor de Emilio, the big brother of Emilio” and so forth) throughout all his appearances in the entire series of films. That is, he is always Álvaro throughout the narrative and as the facts unfold they are treated as a valid history.
How are such mappings achieved by language learners and in discourse in general? And, equally, why do they seem to be so important to comprehension of language?
Language and Genetics
Bertrand Russell, a leading philosopher of the 20th century once poked fun at the notion that words have special powers. However, it was Russell who insisted on a deep relation between the meaning and truth of words (1950). He saw meaning as more basic and in this idea argued against Hans Reichenbach (1938) who took truth value to be more basic and meaning to be dependent. As soon as I read their arguments, I knew that both were very close to discovering the necessary basis for language acquisition. Imagine Russell’s reaction to the discovery of the “genetic code” in the mid 1950s. It was a serious game changer because it was no longer possible to argue that words have nothing to do with the origin(s) of life.
As I would point out in several papers and professional presentations in the late 1970s and throughout the 1980s (e.g., Oller, 1989a), the discovery of the genetic code made words indispensable to the description of life itself. We now know that the “genetic code” is perhaps just the lowest level of a hierarchy of interrelated language systems that are dynamically interacting throughout life. It was during this period that I discussed the hunch that the human language capacity, manifested in the acquisition of proficiency in one or more particular languages, is evidently the main manifestation of human intelligence (Oller, 1981). It is also, as Chomsky (1972) had already argued, and continues to argue to this day, a capacity that appears to be absolutely unique to human beings, though he himself has (Hauser, Chomsky, & Fitch, 2002) tried to suggest ways that the gap between humans and other primates, chimps, for instance, might be bridged by cumulative mutations that suddenly express themselves. We might be reminded of what Gould (1977a, 1977b) described as a “hopeful monster” (a creature very unlike its predecessors and contemporaries). Gould proposed such “saltations” (big jumps) to explain the ubiquitous huge gaps throughout the whole of the fossil record.
The problem pointed to by Hauser, Chomsky, and Fitch (2002), and later by Penn, Holyoak, and Povinelli (2008, 2009), is how to explain the discontinuity between chimps and man not only with respect to the unique human language capacity, but also with respect to all the nonverbal reasoning abilities, especially ones that involve “recursion,” that are also unique to humans.
Chomsky first stressed recursion in the syntax of natural languages. I like to illustrate it in pragmatic terms this way: By about the age of 3 years normal children are able to understand a potentially infinite regression in a story that begins while everyone is sitting around a campfire and someone decides to tell a story and the story begins like this: everyone is sitting around …. and so forth. Human children who are progressing normally, will catch on to the pragmatic recursion early and easily, but none of the higher primates seems capable of the first step in such a regression. Much less can they conceptualize notions such as infinity (or everything), zero (as in nothing at all), past tense, future tense, hypotheticals, conditionals, or complex syntax involving negation, conjunction, and subordination. The best trained signing chimps and gorillas never challenge the use of a word, make comments on comments, or ask questions about what things are called or why. Yet human children can do all these things by some time between their third and seventh birthdays. Why is that?
The 1990s
It would take some time and a good deal of theoretical work to produce intelligible proofs of the logicomathematical kind showing that all language acquisition utterly depends on the kind of pragmatic mapping that occurs in TNRs (Oller, 1993, 1995, 1996a, 1996b). The underlying idea had been hinted at by Augustine around 397 AD. In 1879, mathematician Gottlob Frege suggested that true uses of language were the only sources of meaning, but he did not take the trouble to try to prove it. Actually, sufficient proofs were later produced by C. S. Peirce (1897) as well as Alfred Tarski (1936, 1944), but their applicability to the special problem of child language acquisition, much less to genetics, was not easy to appreciate.
The simplest kind of pragmatic mapping, though it is already complex and too abstract for any nonhuman to fully understand, is the sort found in a name correctly applied to the particular person who goes by that name. For instance, if we intend to refer to the President of the American Civil War by the name Abraham Lincoln, the association of that name with that particular individual of history, would be an example of such a valid pragmatic mapping, a TNR. I first argued that language acquisition depends on precisely that sort of association in 1969, but it would take nearly another quarter of a century before intelligible proofs of that idea could be produced.
In the meantime, another stream of research that I had begun developing while at UCLA and had continued working on at the University of New Mexico was heating up. After ruling out the hypothesis that a general factor of language proficiency might account for all the reliable variance in language based tests, it remained clear from the best refutations of that implausible idea, one that needed to be ruled out before proceeding, that acquired proficiency in one’s best (strongest) language was still accounting for the lion’s share of variance in IQ tests in general, including ones aimed at testing “nonverbal” abilities. Why were the best nonverbal IQ tests more strongly correlated with verbal IQ tests than with each other? It appeared that language/dialect proficiency was the primary factor being measured by such tests rather than “innate intelligence” as had been claimed by Jensen (1969, 1980) and by Herrnstein (1973), and Herrnstein and Murray (1994).
In 1997, I published an article challenging Herrnstein’s theory of the “meritocracy.” He supposed that innate intelligence was the main factor involved in sorting individuals into higher and lower socio-economic brackets. In doing so, he also claimed, along with Jensen and others who were heavily involved in defending the IQ tests as unbiased against persons who do not speak English as their native language, or who do not have the dialect of the tests and testers as their primary dialect of English. In short, they claimed that Blacks get lower scores not because of language/dialect or even socio-economic status (SES), but because they have less innate ability than Whites.
My challenge was strictly on the basis of evidence showing that the language/dialect factor is by far the biggest factor in the tests. Also, attributing differences in test outcomes for Blacks and Whites to the language/dialect factor was a simpler theory and explained the contrasts. Others had shown that the differences could be accounted for on the basis of SES. The counter coming back from Herrnstein was that SES is the primary result of innate intelligence rather than the reverse. So, there was a kind of chicken and egg problem. Which was the cause and which was the result? My answer was to examine the IQ tests more closely and to show on a prima facie basis that they directly measure language/dialect proficiency which is acquired. For persons who do not know the language/dialect of the testing well, or at all, lower scores (all else being equal) cannot reasonably be attributed to “innate” intelligence because that is not what the tests directly assess.
The question would remain incompletely resolved for a few more years, but in the meantime, the editor of the journal where my 1997 paper was to be published insisted that I also deal with “social Darwinism,” an outcropping of the 19th century philosophy that dominates the textbooks recently recommended for Louisiana high school students by the Board of Elementary and Secondary Education (BESE).
On April 26, 1998, Eric Harris wrote about his plan to improve society “by boosting natural selection.” Then, almost a year later after a great deal of planning and forethought, on April 20, 1999, the birthday of the most infamous person of the 20th century, Eric carried out his plan. It would come back to haunt the supporters of Darwin’s 19th century philosophy about the survival of the fittest. In honor of the Darwinian orthodoxy, that person Eric Harris honored had written:
if this law [the Darwinian dogma of natural selection by survival of the fittest] did not prevail, any conceivable higher evolution (Höherentwicklung) of organic living beings would be unthinkable (for discussion see Weikhart, 2009, p. 36; and dozens of other books on this subject).
On the day he and Dylan Klebold acted out his plan, Eric Harris wore a teeshirt emblazoned with the words “NATURAL SELECTION.” The date of the crime, April 20, 1999 would have been the 110th birthday of Adolf Hitler.
Three quarters of a century earlier, Clarence Darrow defended a similar pair of murderers who killed 14 year-old Bobby Franks in 1924. The famous Darrow is said to have given his longest and perhaps his best defense ever pleading against the death penalty for one of his clients. He said:
 This terrible crime was inherent in his organism, and it came from some ancestor… It is hardly fair to hang a 19-year-old boy for the philosophy that was taught him at the university? (Scopes, 1925, pp. 178-179, 182)
This terrible crime was inherent in his organism, and it came from some ancestor… It is hardly fair to hang a 19-year-old boy for the philosophy that was taught him at the university? (Scopes, 1925, pp. 178-179, 182)
According to the historical record, the murderers, Nathan Leopold and Richard Loeb, were extraordinary intellectuals. They were smart enough to connect the dots. One of the spokespersons at the recent discussion of biology texts in Louisiana questioned whether Eric Harris knew enough Darwinian philosophy to apply it by killing 12 students, one teacher, and injuring 21 others on April 20, 1999. How hard is it to see that “survival of the fittest” entails death to anyone less than a Nietzschean superman–the fittest. Adolf Hitler read it that way and hardly ever gave a speech or wrote a treatise in which he did not emphasize the idea that it was the goal of the German people in both of the great wars of the 20th century to kill off the unfit (Wiekart, 2009).
At the Nuremberg War Crimes Tribunal Dr. Leo Alexander, who worked with the Chief American Counsel, explained the view which Hitler attributed directly to the 19th century philosophy of Charles Darwin about the “unfit” which would come to mean anything less than the “fittest.” The Germans came believed:
. . . that there is such a thing as life not worthy to be lived. This attitude in its early stages concerned itself merely with the severely and chronically sick. (1949, p. 45)
The first “unfit” persons on the list to be destroyed were
the mentally defective, psychotics (particularly schizophrenics), epileptics and patients suffering from infirmities of old � age and from various organic neurologic disorders such as infantile paralysis, Parkinsonism, multiple sclerosis and brain tumors. (1949, p. 41)
But the list did not end there:
Gradually, the sphere . . . was enlarged to encompass the socially unproductive, the ideologically unwanted, the racially unwanted, and finally all non-Germans. But is it is important to realize that the infinitely small wedged-in lever from which the entire trend of mind received its impetus was the attitude towards the non-rehabilitatable sick. (1949, p. 45)
It might be possible for the defenders of the 19th century orthodoxy to argue that Hitler was an aberration, as were Leopold and Loeb, Eric Harris and Dylan Klebold, and, in fact, all the German people who followed Hitler like ravenous wolves, starting World War II and killing millions of helpless civilians in addition to military combatants. But for anyone seeking that route to a defense of Darwinian philosophy it would be a good idea to stop a while and read the book by astronomer Fred Hoyle, who wrote:
The modern point of view that survival is all has its roots in Darwin’s theory of biological evolution through natural selection. Harsh as it may seem, this is an open charter for any form of opportunistic behavior. Whenever it can be shown with reasonable plausibility that even cheating and murder would aid the survival either of ourselves personally or the community in which we live, then orthodox logic enjoins us to adopt these practices, just because there is no morality except survival. (1983, p. 8).
2000-2010: The Present Decade
Three years after its first appearance, my paper challenging the theory of the meritocracy (Oller, 1997) would be republished by an invitation from a different editor in the journal of geniuses, Mensa.Although it is not well-known, in his 1874 Descent of Man (2nd edition published in New York by A. L. Burt, Company), Charles Darwin was very explicit in his theory that Blacks are closer to apes than Whites. According to himself, Blacks came down out of the trees a little later. The impact would be felt for more than a century and a half and would reverberate in some of the most dramatic events of all recorded history. Mintz (1972) wrote,
Ab initio, Afro-Americans were viewed by these intellectuals as being in certain ways unredeemably, unchangeably, irrevocably, inferior. (p. 387)
Or as one editor remarked in Science,
That generation of scientists believed that no artificial process of education or forced evolution would ever enable the Blacks to catch up. (p. 506)
At the beginning of the 21st century, however, a logicomathematical argument would be developed showing that “nonverbal” tasks absolutely depend on concepts that are only attainable by acquiring a high degree of proficiency in some natural language (Oller, Kim, & Choe, 2001). It might be English, Chinese, Korean, or pick a language, but to do really abstract nonverbal reasoning, the underlying concepts of some language must be achieved. The proofs show that such acquisition cannot proceed unless certain foundations of a distinctly linguistic sort are laid. Without going into detail, for instance, in order to build up conjoined propositions containing complex argument/predicate relations, it is first necessary to build up the arguments and the predicates. The problem for a person who has no linguistic concepts at all is very much like a person who must build a house of bricks but has not made any bricks yet and has no way to obtain any.
In addition to the logicomathematical proofs (see Oller, Kim, & Choe, 2001) a series of experimental studies with bilinguals (Oller, Kim, & Choe, 2000a, 2000b; Oller, Kim, Choe, & Hernandez, 2001) showed that the best predictor of nonverbal test scores was invariably the stronger language of the bilinguals (Spanish/English and Korean/English), not another nonverbal task of a different sort. These results with bilinguals refute the meritocracy theory as well as the implication drawn from Darwin’s theory about Blacks from his Descent of Man.
Also, the fact that ordinary truth resides only in representations and not in material facts themselves suggests the deeper problem for orthodox biology. The problem is how to get the distinct human capacity to represent any facts truly. Before that, how is it possible for random arrangements of particles of matter first to emerge from nothing, and then to accidentally arrange themselves into the polymer chains necessary to every part of the biosphere. The human language capacity is crucial because without it nothing whatever could be discovered and we would not be having this discussion.
Einstein saw the latter as the greater problem writing:
The eternal mystery of the world is its comprehensibility. (Albert Einstein, 1936, p. 61)
A Racy Theory
The entire scientific discussion of IQ in relation to language/dialect proficiency shows the poverty from a theoretical point of view of the 19th century Darwinian claims about race. It also uncovered the sinister and direct line connection between that 19th century philosophy and the view that Blacks are inferior.
Most Americans are unaware of efforts in the United States to cleanse the “gene pool” (Black, 2003). They do not know about the Eugenics Records Office (ERO) that existed in this country from 1910 until 1939, nor of its association with the Station for Experimental Evolution (SEE—destined to become the prestigious Cold Spring Harbor Lab; also see Allen, 1995; Kamin, 1995a, 1995b; Sedgwick, 1995). Eventually the American Eugenics Office went underground as the Pioneer Fund which supported research leading to the racy claims of Jensen, Herrnstein, and their colleagues. It was they who argued that IQ tests are unbiased measures of innate intellect and that those tests, therefore, show the inferiority of Blacks.
Connecting the circle all the way back to the 19th century philosophy of Darwin, the whole aim of the American Eugenics Movement was to prevent the mingling of supposedly “superior” with “inferior” genes. Hitler wrote in Mein Kampf about “Negroes in the Rhineland” with the aim of “ruining the White race.” He made the connection to Darwin’s 1874 theory of staggered descents from distinct ape ancestors, by writing of “monstrosities halfway between man and ape” and so on. There are so many books and resources on the historical record of Hitler’s use of the 19th century claims about “natural selection” to justify the killing of millions that there is no need to go further. False ideas have ugly consequences. Does killing off the weak actually ensure the advance from ape to man? Is it the source of life and the unique human language capacity and all that goes with it? Is that theory dead and gone? Hardly. Recall Suddendorf’s argument from 2008 in the just prior post about the growing distance, according to him, between man and living primates.
In my just previous post, I already showed how present day biological science disputes any sort of continuity between the unique human language capacity and the communication systems and intellectual abilities of other primates. In fact, according to Suddendorf’s comments on Penn, Holyoak, and Povinelli (2008), the same sort of discontinuity is a pervasive problem across all species. Interestingly, Suddendorf attributed such gaps to the killing off of neighboring but weaker and less fit species. Should the ongoing discussions of current biological science be discussed in biology books for high school students? Or should the 19th century dogma be presented as the absolute unquestionable scientific truth? That is the question that remains.
TNRs at the Basis
In the meantime, sound theory and a great deal of empirical research show that ordinary true reports, TNRs, form the necessary basis for the viability of all life. The most critical properties of TNRs are strictly formal in the sense of mathematical logic and are absolutely unique to TNRs. For one, TNRs are the only representational systems that are sufficiently well-formed to determine anything whatsoever about the material world. This is thedeterminacy property of TNRs. For another, because of their valid mapping onto some particular fact(s) in the material world, TNRs become connected with it and with each other. This is the connectedness property. Finally, because of their connections with actual particulars and thus with the whole scope of the past, present, and future of the material world, TNRs are the only representational systems that validly generalize, exactly to the limit of the similarities of the particular facts which TNRs single out for attention from one context to another. With TNRs the generalizability extends to all possible similars whether they are factual or merely imagined. This is the generalizability property. Sometimes they have been referred to as “perfections” (Oller, 1996a, 1996b), but only in the sense of their being relatively, a formally proved, more complete (all else being equal) than all other systems of representation.
In 2005 and 2007, additional proofs were published (Oller, Chen, Oller, & Pan, 2005; Oller & Chen, 2007) showing that the common chronological order of events in a narrative, where events A, B, C, and so on are reported in the same order as they occurred in corresponding TNRs 1, 2, 3, and so on, where 1 maps to A, 2 maps to B, 3 maps to C, and so on, are universally the simplest possible and (all else being equal) must be the easiest to comprehend, to produce, to recall, and to learn from. This idea was implicit in the Spanish language program written by John Oller Sr. (Oller, Sr., 1963-1967). As noted, he called it, “meaningful sequence.” Later, I would call it “episodic organization” but the idea remains the same. It also would turn out to be (see proofs by Oller & Chen, 2007) the necessary basis for TNRs and for all valid measurement in the sciences.
Are such logicomathematical arguments related to biology? Of course, they are. As we penetrate more and more deeply into the nature of sign systems in general, we are also learning more about how they break down; hence, the connection of all the foregoing to the study of communication disorders (Oller, Oller, & Badon, 2006, 2010; Oller, & Oller, 2010). Fictions in the genome can be seen as unexpressed genes; errors as the basis for genetic disorders such as sickle cell anemia to pick just one where a single misplaced element out of a sequence of some 600 produces the disorder; and lies as viruses that invade organisms and misrepresent their own genetic material as belonging to the invaded organism. Nonsense in biological representations can also be found floating in vaccines that contain fragments of animal proteins that are foreign litter that needs to be expelled from persons injected with them.
Factors interfering with and disrupting TNRs mess up biological communication systems. As demonstrated throughout all the discussions in the posts on this blog, when disruptive influences such as the neurotoxic/genotoxic thimerosal is introduced directly into bodily tissues, communications systems from DNA all the way to human language and its social benefits are tampered with. Throw in some additional toxins, disease agents, foreign animal proteins, viruses, and the like, and should we be surprised to find that we have done harm in producing anaphylactic shock, seizures, Sudden Infant Death Syndrome (also called Sudden Unexpected Infant Death Syndrome by the CDC), gut disease, autism, and too many other disease conditions to name?
The theory of TNRs merely spells out in relation to biochemistry what is obvious at the higher level of social systems. For instance, with respect to high stakes communication in education, commerce, and politics, see Oller and Giardetti (1999). Introducing a lot of false information and noise (random mutations) does not make communication systems more efficient. For that reason, the notion that death and mayhem will naturally (by the death of the unfit) lead from something like an amoeba to a human being can be seen to be a deficient theory. That is why the astronmer, Fred Hoyle, referred to the biological orthodoxy of 19th century Darwinism as “a theory which could be seen to be unworkable” (1983, p. 25). Harvard paleotologist, Stephen Jay Gould put the problem this way:
We fancy ourselves the only true students of life’s history, yet to preserve our favored account of evolution by natural selection we view our data as so bad that we never see the process we profess to study (1977a, p. 14).
If Darwin’s theory were proposed by anyone as an explanation of language acquisition by human children, say, that they learn languages by being randomly mutated and naturally selected for survival or extinction, that theory would just be regarded as absurd. So, here is my question: Why is it unscientific to challenge the Darwinian orthodoxy? What special privilege makes it “the only trajectory” of modern thought that is allowable.
I am reminded of the conversation between Hugh Grant and Sandra Bullock in Two Week’s Notice. She says he is the “most selfish human being on the planet” to which he responds, “Why that’s just silly. Have you met everyone on the planet?” Have the proponents of Darwin’s blunt, blind, and mute tools of random change and killing off of the unfit actually examined all other possible lines of thought?
References
Allen, G. E. (1995). Eugenics comes to America. In Jacoby and Glauberman (1995, 441-475).
Black, Edwin. (2003). War against the weak: Eugenics and America’s campaign to create a Master Race. New York/London: Four Walls Eight Windows.
Bloomfield, Leonard. (1933). Language. New York: Holt, Rinehart, and Winston.
Chomsky, Noam A. (1957). Syntactic structures. The Hague: Mouton.
Chomsky, Noam A. (1972). Language and mind. New York: Harcourt.
Chomsky, Noam A. (1995). Language and nature. Mind, 104, 1-61.
Darwin, Charles. (1874). The descent of man. Second edition. New York: D. Appleton.
Einstein, Albert. (1936). Physics and reality. In Out of my later years, author. Secaucus, New Jersey: Citadel, pp. 59-96. Abridged and reprinted in Oller (1989b, 3-11).
Einstein, Albert. (1941). The common language of science. In Out of my later years, author. Secaucus, New Jersey: Citadel, 1956, pp. 111-113. Reprinted in Oller (1989b, 61-65).
Frege, G. (1967). Begriffsschrift, a formula language, modeled upon that of arithmetic, for pure thought. In J. van Heijenoort (Ed.), From Frege to Gödel: A sourcebook in mathematical logic (pp. 5-82). Cambridge, Massachusetts: Harvard University Press. (Originally published 1879)
Gould, Stephen J. (1977b). This view of life: The return of hopeful monsters. Natural History 86(6), 22, 24, 28, 30.
Gould, Stephen J. (1977a). This view of life: Evolution’s erratic pace. Natural History 86(5), 12, 14, 16.
Hauser, Marc D., Chomsky, Noam A., & Fitch, W. Tecumseh. (22 November, 2002). The faculty of language: Who has it? How did it evolve? Science, 298(5598), 1569-1579. DOI: 10.1126/science.298.5598.1569
Herrnstein, R. J. (1973). IQ in the meritocracy. Boston: Atlantic-little Brown.
Herrnstein, R. J., & Murray, C. (1994). The bell curve: Intelligence and class structure in American life. New York: Free Press.
Jacoby, R. and Glauberman, N. (Eds.), (1995). The bell curve debate: History, documents, opinions. New York: Random House.
Jensen, A. R. (1969). How Much can we boost IQ and scholastic achievement? Harvard Educational Review 39, 1-123.
Jensen, A. R. (1980). Bias in mental testing. New York: Free Press.
Kamin, L. (1995a). Lies, damned lies, and statistics. In Jacoby and Glauberman (1995, 81-105).
Kamin, L. (1995b). ‘The pioneers of IQ testing. In Jacoby and Glauberman (1995, 476-509).
Oller, J. W., Jr. (1970). Transformational theory and pragmatics. Modern Language Journal, 54, 504-507.
Oller, John W., Jr. (1989a). Conclusions toward a rational pragmatism. In Oller (1989b, 223-250).
Oller, J. W., Jr. (1975). Pragmatic mappings. Lingua, 35, 333-344.
Oller, J. W., Jr. (1981). Language as intelligence? Language Learning, 31, 465-492.
Oller, J. W., Jr., (Ed.), (1989b). Language and experience: Classic pragmatism. Lanham, Maryland: University Press of America.
Oller, J. W., Jr. (1993). Reasons why some methods work. In J. W. Oller, Jr. (Ed.),Methods that work: ideas for literacy and language teachers (pp. 374-385). Boston, MA: Heinle and Heinle.
Oller, J. W., Jr. (1995). Adding abstract to formal and content schemata: Results of recent work in Peircean semiotics. Applied Linguistics, 16(3), 273-306.
Oller, J. W., Jr. (1996a). How grammatical relations are determined. In B. Hoffer (Ed.) The 22nd Linguistic Association of Canada and the United States (LACUS) forum, 1995 (pp. 37-88). Chapel Hill, North Carolina: Linguistic Association of Canada and the United States (series Ed., T. Griffen).
Oller, J. W., Jr. (1996b). Semiotic theory applied to free will, relativity, and determinacy: Or why the unified field theory sought by Einstein could not be found. Semiotica,108(3/4), 199-244.
Oller, J. W., Jr. (2000). Monoglottosis: What’s wrong with the idea of the meritocracy and its racy cousins? Mensa Research Journal, 45, 10-48. Reprinted by invitation from Oller (1997), Applied Linguistics, 18 (4), 467-507.
Oller, J. W., Jr. & Chen, Liang. (2007). Episodic organization in discourse and valid measurement in the sciences. Journal of Quantitative Linguistics, 14, 127-144.
Oller, J. W., Jr., Chen, L., Oller, S. D., and Pan, N. (2005). Empirical predictions from a general theory of signs. Discourse Processes, 40(2), 115-144.
Oller, J. W., Jr. & J. Giardetti, J. R. (1999). Images that work: Creating successful messages in marketing and high stakes communication. Westport, Connecticut: Quorum Books.
Oller, J. W., Jr., Harrington, R. V., & Sales, B. D. (1969). A basic circularity in traditional and current linguistic theory. Lingua, 22, 317-328.
Oller, J. W., Jr., Kim, K., & Choe, Y. (2000a). Applying general sign theory to testing language (verbal) and nonverbal abilities. Language Testing, 17(4), 377-396.
Oller, J. W., Jr., Kim, K. & Choe, Y. (2000b). Testing verbal (language) and nonverbal abilities in language minorities: A socio-educational problem in historical perspective.Language Testing, 17(3), 341-360.
Oller, J. W., Jr., Kim, K., & Choe, Y. (2001). Can instructions to nonverbal IQ tests be given in pantomime? Additional applications of a general theory of signs. Semiotica, 133(1/4), 15-44.
Oller, J. W., Jr., Kim, K., Choe, Y., & Hernandez-Jarvis, Lorna. (2001). Testing verbal (language) and nonverbal abilities in children and adults acquiring a nonprimary language.Language Testing, 18(1), 33-54.
Oller, J. W., Jr., & Obrecht, Dean H. (1968). Pattern drill and communicative activity: A psycholinguistic experiment. International Review of Applied Linguistics, 6, 165-174.
Oller, J. W., Jr., & Obrecht, Dean H. (1969). The psycholinguistic principle of informational sequence: An experiment in second language learning. International Review of Applied Linguistics, 7, 165-174.
Oller, J. W., Jr., & Oller, S. D. (2010). Autism: The diagnosis, treatment, and etiology of the undeniable epidemic. Sudbury, MA: Jones and Bartlett Publishers.
Oller, J. W., Jr., Badon, L. C., & Oller, S. D. (2010). Cases: Introducing communication disorders across the life span. San Diego, CA: Plural Publishing, Inc.
Oller, J. W., Jr., Oller, S. D., & Badon, L. C. (2006). Milestones: Normal speech and language development across the life span. San Diego, CA: Plural Publishing, Inc.
Oller, J. W., Jr., & Sales, B. D. (1969). Conceptual restrictions on English: A psycholinguistic study. Lingua, 23, 209-232.
Oller, J. W., Sr. (1963-1967). El espaňol por el mundo (La Familia Fernandez, Primer Nivel; Emilio en España, Segundo Nivel; Coloquios Culturales, Field Test Edition). Chicago: Encyclopedia Britannica Films, Inc.
Patterson, Colin. (1981). Interviewed by Brian Leith. The Listener, 106, 390.
Peirce, C. S. (1897). The logic of relatives. The Monist, 7, 161 – 217. Also in C. Hartshorne & P.Weiss (Eds), (1932), Collected Papers of C. S. Peirce, Volume 2 (pp. 288 – 345). Cambridge, MA: Harvard University Press.
Penn, D. C., Holyoak, K. J., & Povinelli, D. J. (2008). Darwin’s mistake: Explaining the discontinuity between human and nonhuman minds. Behavioral & Brain Sciences, 31, 109-178. DOI:10.1017/S014525X08003543
Penn, D. C., Holyoak, K. J., & Povinelli, D. J. (2009). Universal grammar and mental continuity: Two modern myths. Behavioral & Brain Sciences, 32(5), 462-464. DOI:10.1017/S014525X09990719
Reichenbach, Hans. (1938). Experience and prediction: An analysis of the foundations and the structure of knowledge. Chicago, IL: University of Chicago Press.
Russell, Bertrand. (1950). An inquiry into meaning and truth. London: George Allen & Unwin.
Scopes, J. T. (1925). World’s greatest court trial. Cincinnati : National Book Co.
Sedgwick, John. (1995). Inside the Pioneer Fund. In Jacoby and Glauberman (1995, 144-161).
Suddendorf, T. (2008). Explaining human cognitive automorphies. Behavioral & Brain Sciences, 31, 147-148. DOI:10.1017/S014525X08003737
Tarski, A. (1956). The concept of truth in formalized languages. In J. J. Woodger (Ed. and Trans), Logic, semantics, and metamathematics (pp. 152–278). Oxford, England: Oxford University. (Originalwork published 1936)
Tarski, A. (1949). The semantic conception of truth. In H. Feigl &W. Sellars (Eds.),Readings in philosophical analysis (pp. 341–374). New York: Appleton. (Original work published 1944)
Weikart, Richard. (2009). Hitler’s ethic: The Nazi pursuit of evolutionary progress. New York: St Martin’s Press (Palgrave Macmillan).


 Vaccine components still include (1) thimerosal (also known as Merthiolate, or in the British spelling, thiomersal), (2) aluminum (a toxin used to jump start the infant’s immune defense systems), (3) formaldehyde, (4) yeast additives, and (5) many different “adventitious” contaminants consisting of foreign animal protein fragments, viruses such as Simian Virus 40 (SV40), the virus that causes “wasting disease” in pigs, and many others that keep turning up. As biochemical assays are improved more and more of the former unknowns are being found in widely used vaccines. The contaminants are ones that come into the vaccines through manufacturing processes that often require routing through the biosystems of a chicken, sheep, pig, cow, or monkey.
Vaccine components still include (1) thimerosal (also known as Merthiolate, or in the British spelling, thiomersal), (2) aluminum (a toxin used to jump start the infant’s immune defense systems), (3) formaldehyde, (4) yeast additives, and (5) many different “adventitious” contaminants consisting of foreign animal protein fragments, viruses such as Simian Virus 40 (SV40), the virus that causes “wasting disease” in pigs, and many others that keep turning up. As biochemical assays are improved more and more of the former unknowns are being found in widely used vaccines. The contaminants are ones that come into the vaccines through manufacturing processes that often require routing through the biosystems of a chicken, sheep, pig, cow, or monkey. Figure 4")






{kind=link}
{kind=link}